Efficacy of Penile Traction Therapy Using andropeyronie device
ANDROPEYRONIE is the only FDA registered and patented penis extender device sold in the US
Efficacy of Penile Traction Therapy Using andropenis device https://clinicaltrials.gov/Sponsor: Mayo Clinic
The safety and scientific validity of this study is the responsibility of the study sponsor and investigators. Listing a study does not mean it has been evaluated by the U.S. Federal Government. Know the risks and potential benefits of clinical studies and talk to your health care provider before participating. Read our disclaimer for details.
Brief Summary:
This clinical trial is designed to assess the safety, dosing, and preliminary efficacy of a novel penile traction device (andropeyronie) on correcting deformities relating to Peyronie's disease, a condition which results in penile curvature and length loss. The trial is designed as a randomized, placebo-controlled study with men randomized to receiving no therapy or penile traction therapy 30 minutes once, twice, or three times daily. The study will occur over a 3 month period, after which an open label phase for 3 months will be conducted. Final assessments for adverse effects will also be assessed at 9 months. Condition or disease Intervention/treatment Phase Penile Diseases Device: ANDROPEYRONIE PTT - randomized and open label Device: ANDROPEYRONIE PTT - open label phase only Not Applicable
Detailed Description: Peyronie's disease (PD) is a fibrotic condition of the penis, affecting 1-13% of the US male population. The disease results in penile curvature and significant psychosocial bother. Current preferred therapies for PD include repeated penile injections with bacterial enzymes and surgery. However, these therapies are expensive and in some cases result in permanent reductions in penile length and sensation. Penile traction therapy PTT (andropeyeonie) is a relatively newer treatment which has been proposed as a treatment for PD with preliminary data suggesting a potential role. However, currently available PTT devices are primarily designed for penile lengthening and have many significant limitations including a requirement of use for 9 hours daily and significant difficulties in personal application. Given these limitations, a new penile traction device (Andropenis) was created and funded through ANDROMEDICAL and was specifically designed to treat men with PD. The primary objective of the current study is to evaluate safety of the device using various dosing schedules, with secondary endpoints designed to assess efficacy and subjective outcomes. To accomplish the study, a population of men from Mayo Clinic with PD will be enrolled and will be randomized to utilize the device for varying amounts of time. Outcomes will be assessed at 3, 6, and 9 months, and results are to be used with the intent to publish in a scientific journal.
Study Type : Interventional (Clinical Trial) Estimated Enrollment : 120 participants Allocation: Randomized Intervention Model: Factorial Assignment Intervention Model Description: Men will be randomized into one of four groups: no traction therapy, penile traction (ANDROPEYRONIE) 30 minutes once daily, penile traction (ANDROPEYRONIE)30 minutes twice daily, and penile traction 30 minutes three times daily. This treatment will continue for 3 months, after which men will enter an open label phase for 3 months. Primary and secondary outcomes will be evaluated at the completion of the 3 month and 6 month time points. Additional AEs will be assessed at 9 months after study initiation. Masking: Double (Investigator, Outcomes Assessor) Masking Description: Objective outcomes including penile length and curvature will be masked for the investigator and outcome assessor by obtaining photographs of the penis in the lateral and dorsal planes. Curvatures will also be assessed by a clinician in the case where photographs are not able to be obtained or if the participant refuses photographs. These will be assessed without any knowledge as to which grouping the patient is located by two independent reviewers. If there are differences >5 degrees (curvature), or 0.5 cm (length), a 3rd individual will mediate the difference. Primary Purpose: Basic Science Official Title: Efficacy of Penile Traction Therapy Using a ANDROPEYRONIE : A Controlled, Single-blinded, Randomized Trial Actual Study Start Date : October 2, 2017 Estimated Primary Completion Date : April 30, 2019 Estimated Study Completion Date : April 30, 2019
Sham Comparator: Group 1 - Control
No treatment will be administered for the initial 3 months. This are is necessary as Peyronie's disease may result in changes in length and curvature as a function of the disease process. After the 3 month period of time, this group will enter an open label phase where they may utilize a penile traction device (andropeyronie) if desired.
xperimental: Group 2 - PTT 1x daily x 3 months
Men will utilize penile traction therapy (andropeyronie) for 30 minutes once daily for the initial 3 months. After this phase is completed, they will enter an open label phase for 3 months where they may utilize the device as much or as little as desired.
Experimental: Group 3 - PTT 2x daily x 3 months
Men will utilize penile traction therapy (andropeyronie) for 30 minutes twice daily for the initial 3 months. After this phase is completed, they will enter an open label phase for 3 months where they may utilize the device as much or as little as desired.
Experimental: Group 4 - PTT 3x daily x 3 months
Men will utilize penile traction therapy (andropeyronie) for 30 minutes three times daily for the initial 3 months. After this phase is completed, they will enter an open label phase for 3 months where they may utilize the device as much or as little as desired.
Primary Outcome Measures :
Number of participants with treatment-related adverse events as reported by participants and evaluated based on physical examination. [ Time Frame: From baseline to 9 months ]Safety as assessed through investigator or individual reporting of adverse events and physical examination with the (andropeyronie) device when used 30 min 1x, 2x, 3x per day and in an open label fashion Secondary Outcome Measures :
Stretched penile length (andropeyronie) - randomized phase [ Time Frame: 3 months duration - from time 0 to 3 months ]Compare changes in stretched penile length following completion of 3 months of (andropeyronie) therapy
Penile curvature - randomized phase [ Time Frame: 3 months duration - from time 0 to 3 months ]Compare changes in penile curvature following completion of 3 months of (andropeyronie) therapy
Stretched penile length (andropeyronie) - open label phase [ Time Frame: 3 months duration - from 3 months after initiation to 6 months ]Compare changes in stretched penile length following completion of the open label phase (beginning 3 months after study initiation and continuing until 6 months) of (andropeyronie) therapy
Penile curvature - open label phase [ Time Frame: 3 months duration - from 3 months after initiation to 6 months ]Compare changes in penile curvature following completion of the open label phase (beginning 3 months after study initiation and continuing until 6 months) of (andropeyronie) therapy
Penile curvature - randomized and open label phase [ Time Frame: 6 months duration - from baseline to 6 months ]Compare changes in penile curvature from baseline until end of open-label phase
Penile length - randomized and open label phase [ Time Frame: 6 months duration - from baseline to 6 months ]Compare changes in penile length from baseline until end of open-label phase
Subjective questionnaire outcomes [ Time Frame: Baseline, 3 months, 6 months ]Compare outcomes of subjective responses to the Peyronie's disease questionnaire (PDQ)
Subjective outcome of erectile function with IIEF [ Time Frame: Baseline, 3 months, 6 months ]Compare outcomes of the International Index of Erectile Function Questionnaire
Subjective outcome of erectile function with SEP2 and 3 [ Time Frame: Baseline, 3 months, 6 months ]Compare outcomes of subjective reporting of the standardized sexual encounter profile questions 2 and 3
Comparison to other treatments [ Time Frame: 3 months, 6 months ]Compare satisfaction with (andropeyronie) to alternative forms of penile traction therapy and other Peyronie's disease therapies through use of a non-standardized set of questions.
Subjective reporting of penile length [ Time Frame: Baseline, 3 months, 6 months ]Comparison of changes in penile length at various time points and among treatment arms
Subjective reporting of penile curvature [ Time Frame: Baseline, 3 months, 6 months ]Comparison of changes in penile curvature at various time points and among treatment arms
MEDICAL PEYRONIE EXTENDER A simple & effective penis curvature correction.
@andropeyronie Correction of curved penis: up to 60% correction of penile curvature caused by Peyronie’s disease ANDROPEYRONIE is the only FDA registered and patented penis extender device sold in the US
Penile traction therapy in Peyronie’s disease ANDROPEYRONIE
Penile traction therapy in Peyronie’s disease (andropeyronie)
Penile traction therapy (andropeyronie) has traditionally been implemented to increase penile length but has recently been investigated for reducing the curvature associated with Peyronie’s disease. The results of a few initial investigations have been conflicting, and further research is needed to confirm the true benefit of such therapy and its potential role in treating Peyronie’s disease as both a monotherapy and in combination with other therapeutic options.
Introduction and context
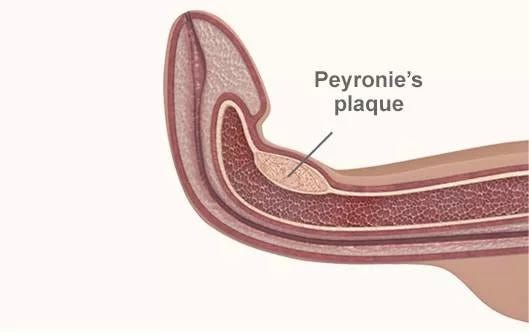
Peyronie’s disease (PD) is a connective tissue disorder involving the tunica albuginea layer of the penis. The fibrotic process that occurs may result in the formation of plaque, one of the classic findings on physical examination of the patient. Men afflicted by this disorder may present with pain, deformity (such as penile curvature or penile shortening) and/or erectile dysfunction (ED). While surgical therapy has been the standard definitive treatment for penile curvature associated with PD, less invasive options have been sought. Aside from the common risks associated with surgical procedures, corrective surgery for the penile curvature associated with PD can result in further penile shortening and worsening penile rigidity with erection [1–4]. Medical options are attractive due to their potential to avoid invasive procedures of the penis, to affect all aspects of the disease, and to intervene before the disease has stabilized and is no longer reversible. However, no single medical treatment has been definitively proven to offer a significant benefit in a large placebo-controlled trial [5,6]. In addition, no medical or surgical therapy offers the benefit of increased penile length to men with PD, a common sequela of the disease and one that can cause significant emotional distress.
While the search for an effective non-surgical therapy for PD has continued, interest in the use of external mechanical force has arisen. The use of a vacuum erection device (VED) has been recommended as an option for treatment of the shortening, curvature, and ED associated with PD. It has also been investigated as an adjunctive therapy to be used in combination with surgical treatment of PD [7]. To date, no large multi-center controlled trial has been performed to validate the use of a VED in these situations.
While the use of traction therapy (andropeyronie) in PD may be a relatively new concept, it has a long history of use in other areas of medicine. In 1969, Ilizarov and Soibeman [8] described ‘distraction osteogenesis’ as a technique to stimulate bone remodeling. Subsequently, the use of traction (andropeyronie) and tissue expansion therapy has spread to other areas, including orthodontics and plastic/reconstructive surgery [9]. From these initial experiences, the concept of using traction therapy (andropeyronie) to lengthen the penis was felt to be a logical consideration. In 2001, Scroppo and colleagues [10] reported the results of a small study that investigated the use of penile traction (andropeyronie) to treat PD curvature. Eight men with PD and no complaints of ED were instructed to use a penile traction device (andropeyronie) for at least 4 hours per day for a total treatment period of 3–6 months. The authors reported a statistically significant decrease in mean erect curvature of 14° (from 34 to 20°). However, this study involved a very small cohort of patients with no control group.
Several years later, Moncada-Iribarren and colleagues [11] reported on the use of a traction device (andropeyronie) to treat penile shortening that had occurred after PD surgery. A total of 40 men participated in this study, with 12 undergoing a grafting procedure while the remaining 28 underwent plication only. One-half of the patients were treated with penile traction (andropeyronie) and the other half served as the control group. The penile extender was first instituted once the surgical incision had healed (approximately 2–3 weeks) for 8–12 hours daily for a total treatment period of at least 4 months. For both groups, penile shortening after surgery ranged from 0.5–4.0 cm. Those patients in the treatment group experienced a length increase ranging from 1–3 cm and this increase was proportional to the number of hours per month that the patient was wearing the extender (andropeyronie). The authors also studied the potential impact of the device (andropeyronie) on the quality of life of their study groups and identified significant differences in several parameters for the patients using the device versus those in the control group.
Recent advances
Based on these initial positive studies, further investigation into the use of penile traction(andropeyronie) as a non-surgical alternative in the treatment of PD deformity was encouraged. In 2008, Levine and colleagues [12] reported the results of a study of 11 men with PD who underwent treatment with a penile traction device (andropeyronie). All participants were evaluated with pre-treatment measurement of stretched penile length from pubis to corona, and a dynamic color duplex ultrasound was performed with measurement of curvature and girth at maximal erection. Of the 11 men who entered the study, one subject dropped out due to inability to comply with the treatment protocol. Patients were instructed to wear the device for a minimum of 2 hours per day but were encouraged to increase the duration of use to a maximum of 8 hours per day. Treatment was continued for a total of 6 months. Every 2 weeks, the extender rods were lengthened by 0.5 cm, and repeat length measurements were recorded every month during an office visit.
Of the 10 men who completed the study, all reported subjective improvements in length and curvature of 0.5–2.5 cm and 10–40°, respectively. Objectively, mean penile stretched length increased from 0.5–2.0 cm and curvature had been reduced by 10–45° (mean of 22°). There were no patient-described changes regarding penile sensation, worsening erectile function, or skin injury. Overall, patients reported high satisfaction rates and improvements in International Index of Erectile Function (IIEF) scores.
This year, Gontero and colleagues [13] published the results of a study of 19 men who underwent treatment with a penile traction device(andropeyronie) for PD-associated penile curvature. Of the men participating, all had pre-treatment curvature of less than 50°, disease lasting a minimum of 12 months, and no penile pain when flaccid. In contrast to the Levine study, measurements of curvature were determined by photography taken by the investigators after a pharmacologically induced erection in the office or, for patients who refused, by auto-photography at home. Patients were required to wear the device (andropeyronie) for a minimum of 5 hours daily, up to a maximum of 9 hours. Patients were evaluated at months 1, 3, and 6. After finishing treatment at month 6, they were evaluated again at 12 months (washout period of 6 months). A total of four patients were dropped from the final analysis due to lack of compliance with the protocol or were lost to follow-up. For the remaining 15 patients available for analysis, median daily use of the device was 5.5 hours. Penile curvature decreased, from a mean of 31°, to 27°. Although this was not statistically significant, there was a significant improvement in mean flaccid and stretched penile length measurements of 1.3 and 0.83 cm, respectively. No further changes in curvature or length were noted after the washout period. There was only a marginal improvement in IIEF score, which was also not statistically significant.
There are several potential explanations for the large discrepancies in the findings between the Levine and Gontero studies. The selection criteria for each study were quite different. For example, the Gontero study required all patients to have the stable form of the disease, which possibly meant that this patient group had disease symptoms that were less amenable to therapy. The Gontero study also limited their study group to patients with curvature of less than 50°, which may have reduced the potential impact of traction therapy. In addition, it is difficult to compare changes in IIEF scores as the treatment group from both studies differed in their baseline scores. Treatment protocol and methods of evaluation were not kept constant across both studies.
Implications for clinical practice
While the value of traction forces in treating various medical conditions has been established, its role in the treatment of the deformities associated with PD has yet to be defined. Initial studies have indicated a role in promoting recovery of penile length lost as a result of the disease. More recent investigations have validated this, although a large controlled trial has yet to be performed. Of the few studies that have been done, contrasting evidence exists as to how beneficial a traction device may be for improving penile curvature. While some mild to moderate improvement may be anticipated, a lack of uniformity in the evaluation of patients across these studies causes the results to be difficult to interpret. Until uniform methods of evaluating PD patients are agreed upon across these studies, a definitive answer will be difficult to reach [14].
As the search for effective non-surgical therapies for PD continues, some have proposed a role for ‘combination therapy’, with traction therapy being a potential component. In fact, Abern and Levine [15] reported on such a protocol in a study of 71 men. In this non-controlled study, a greater improvement in penile curvature was seen in those patients who elected to undergo verapamil injection along with penile traction therapy as opposed to those who underwent injection therapy alone. Again, no definitive recommendations for changes in clinical practice can be made from these findings, but similar studies are forthcoming. Until these investigations involve larger cohorts in a controlled study, it will continue to prove difficult for definitive recommendations to be made.
The investigation of the use of traction therapy in treating men with PD is still in its infancy. Although no large multi-center controlled trials have been published to date, the initial reports are promising. Whether traction therapy will prove beneficial as a monotherapy or in combination with other therapies remains to be seen. At this point, penile traction appears to be a safe and potentially effective option for men wishing to minimize loss of length after corrective surgery for PD. It may also be a reasonable alternative for men who are not candidates for surgery or refuse surgery, and who are wishing to seek modest improvements in recovery of length and penile curvature.
The author declares that he has no competing interests.
References
1Van Der Horst C, Martinez Portillo FJ, Seif C, Alken P, Juenemann KP: Treatment of penile curvature with Essed-Shroeder tunical plication: aspects of quality of life from the patient’s perspective. BJU Int. 2004, 93:105–08.PubMed | CrossRef2Syed AH, Abbasi Z, Hargreave TB: Nesbit procedure for disabling Peyronie’s curvature: a median follow-up of 84 months. Urology. 2003, 61:999–1003.PubMed | CrossRef3Greenfield JM, Lucas S, Levine LA: Factors affecting the loss of length associated with tunica albuginea plication for correction of penile curvature. J Urol. 2006, 175:238–41.PubMed | CrossRef4Breyer BN, Brant WO, Garcia MM, Bella AJ, Lue TF: Complications of porcine small intestine submucosa graft for Peyronie’s disease. J Urol. 2007, 177:589–91.PubMed | CrossRef5Greenfield JM: Peyronie’s disease: options in pharmacologic management. Exp Review Clin Pharm. 2008, 1:299–306.CrossRef6Gholami SS, Gonzalez-Cadavid NF, Lin CS, Rajfer J, Lue TF: Peyronie’s disease: a review. J Urol. 2003, 169:1234–41.PubMed | CrossRef7Lue TF, El-Sakka AI: Lengthening shortened penis caused by Peyronie’s disease using circular venous grafting and daily stretching with a vacuum erection device. J Urol. 1999, 161:1141–4.PubMed | CrossRef8Ilizarov GA, Soibeman LM: Clinical and experimental data on bloodless lengthening of lower extremities. Eksp Khir Anesteziol. 1969, 14:2D–8D.PubMed9Messina A, Messina J: The continuous elongation treatment by the TEC device for severe Dupuytren’s contracture of the fingers. Plast Reconstr Surg. 1993, 92:84–90.PubMed | CrossRef10Scroppo FI, Mancini M, Maggi M, Colpi GM: Can an external penis stretcher reduce Peyronie’s penile curvature?Int J Impot Res. 2001, 13 (Suppl 4). 11Moncada-Iribarren I, Jara J, Martinez-Salamanca JI, Cabello R, Hernandez C: Managing penile shortening after Peyronie’s disease surgery. J Urol. 2007, 177 (Suppl 4):252.12Levine LA, Newell M, Taylor FL: Penile traction therapy for treatment of Peyronie’s disease: A single-center pilot study. J Sex Med. 2008, 5:1468–73.PubMed | CrossRef13Gontero P, Di Marco M, Giubilei G, Bartoletti R, Pappagallo G, Tizzani A, Mondani N: Use of penile extender device in the treatment of penile curvature as a result of Peyronie’s disease. Results of a phase II prospective study. J Sex Med. 2009, 6:558–66.PubMed | CrossRef14Levine LA, Greenfield JM: Establishing a standardized evaluation of the man with Peyronie’s disease. Int J Impot Res. 2003, 15 (Suppl 5):S103–12.PubMed | CrossRef15Abern MR, Levine LA: Intralesional verapamil injections with and without penile traction and oral therapies for management of Peyronie’s disease. J Urol. 2008, 179 (Suppl 4):408.PubMed | CrossRef
Top 3 Penis Extenders For Length Gains As you may know, I’ve spent the last few years testing out different brands of Male Enhancement Supplements . More recently, I’ve been looking for natural and safe ways to increase my penis size. From my research, I discovered Penis Stretchers. If you’re unhappy, with the length of your penis then these devices can help. There are lots of brands for sale online but only a few have been clinically proven and are safe to use. After lots of research, I decided to order a few different devices. I did this to test for quality, comfort, and the potential for success. One of the devices was the most comfortable, and I used it every day for 4 months. Based On My Research and Testing These are The Best Penile Stretchers For Increasing The Length of Your Penis: ANDROPENIS — ANDROEXTENDER — ANDROPEYRONIE ANDROMEDICAL PENIS EXTENDERS After weeks of research online I came up with a short list of 3 penis extenders to choose from. ...
Would You Like An 8.7 Inch Penis? The AndroPenis Penis Extender is Quicker, Easier, More Comfortable & Guarantees Extra Inches!* The most powerful penis enlargement device on the market. Extreme results or double your money back! The original ANDROPENIS (20 years) is the only FDA registered and patented penis extender device sold in the US. Be careful dont buy fakes¡ It’s important to note that results do vary on an individual basis <img class="progressiveMedia-noscript js-progressiveMedia-inner" src="https://cdn-images-1.medium.com/max/1000/1*gVIVXDQz8iW6C81BvecPSQ.jpeg"> andropenis penis extender Safe, Comfortable, Non-Surgical Penis Extension In The Comfort Of Your Own Home Really Is Possible! <img class="progressiveMedia-noscript js-progressiveMedia-inner" src="https://cdn-images-1.medium.com/max/1000/1*K7kTUOGf-FGI7bCb1q4O6Q.png"> andropenis penis extender You want to extend your penis by inches, of ...






Comentarios
Publicar un comentario